Diabetic Foot Ulcer Not Healing? The Problem May Be in Your Arteries — Not Your Wound
Every diabetic patient knows the fear of a foot wound that simply refuses to close.
You clean it. You dress it. You follow every instruction. But weeks pass — sometimes months — and the ulcer stays open. Or worse, it slowly grows.
What most patients and even many families don’t realise is this — a wound cannot heal if adequate blood is not reaching it. And in diabetic patients, blocked or severely narrowed leg arteries are one of the most common — and most underdiagnosed — reasons a foot ulcer refuses to heal.
This is not a wound care problem. This is a vascular problem
The Connection Between Diabetes and Blocked Leg Arteries
Diabetes doesn’t just affect blood sugar. Over years, persistently high glucose damages the inner walls of blood vessels — a process called diabetic vasculopathy. This accelerates the buildup of plaques inside the arteries, gradually narrowing or completely blocking blood flow to the feet and legs.
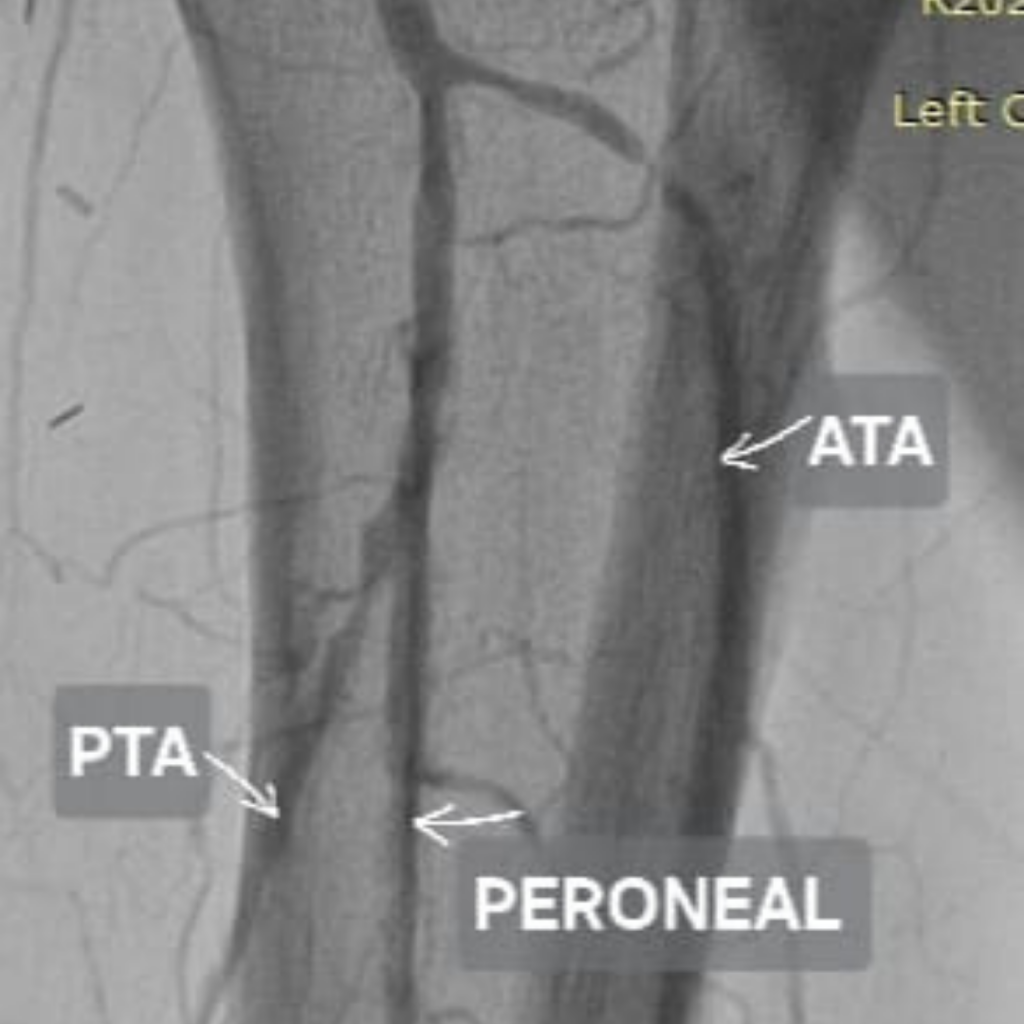
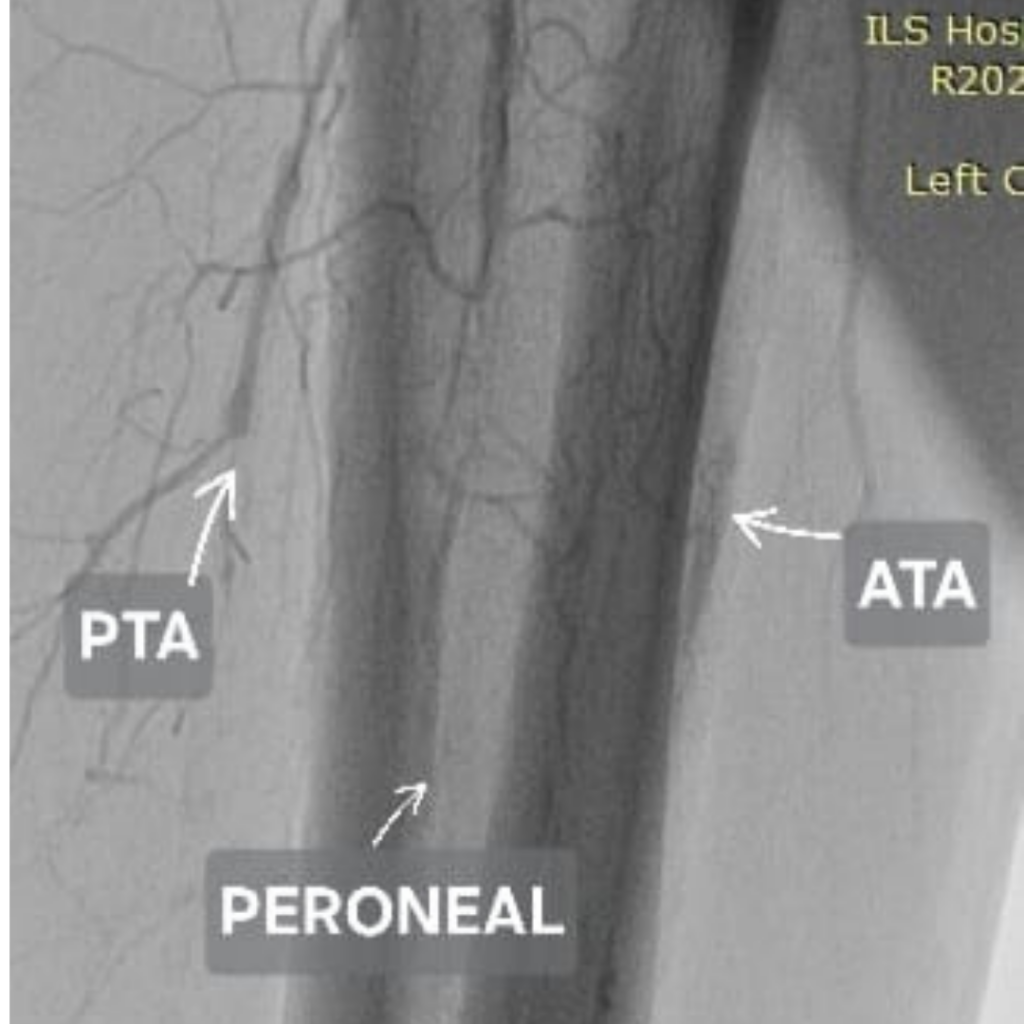
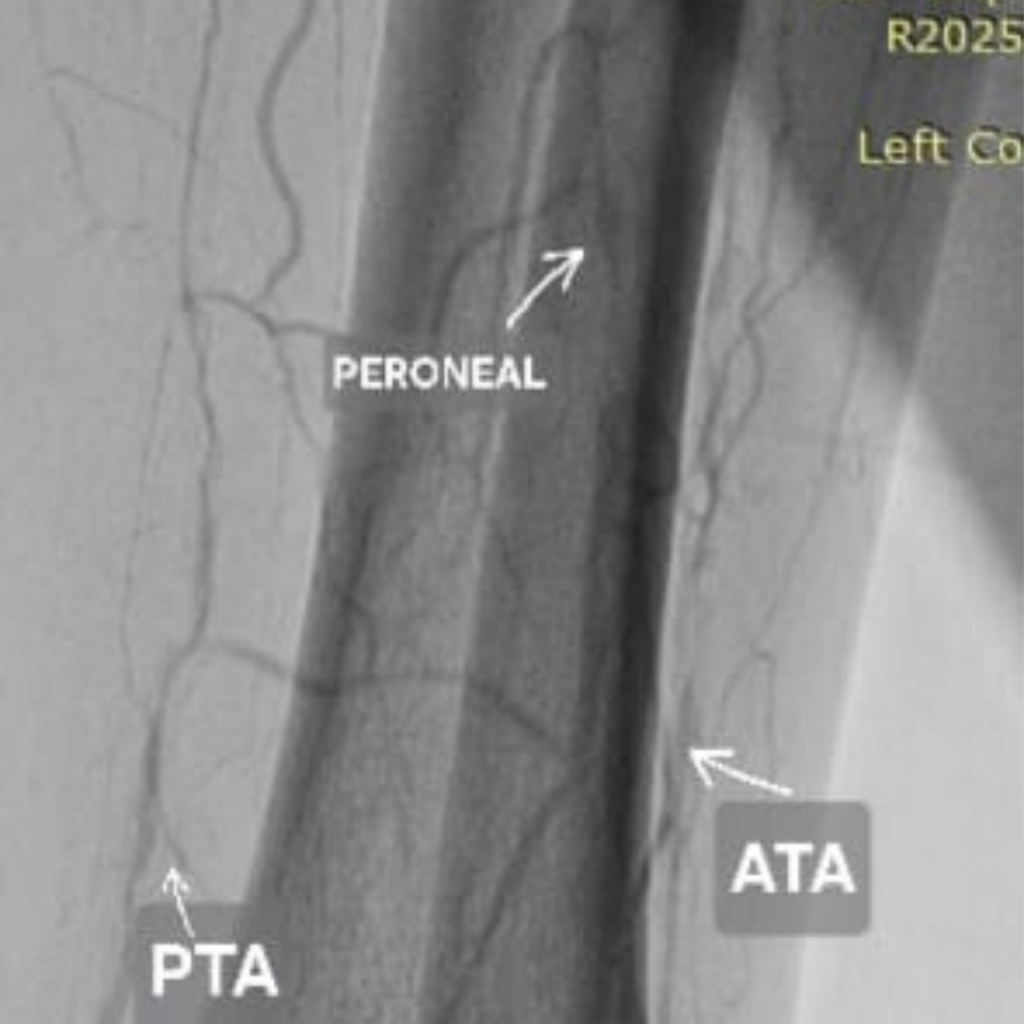
This condition is called Peripheral Artery Disease (PAD) — and in diabetic patients, it tends to affect the smaller arteries below the knee, particularly the
● Anterior Tibial Artery (ATA)
● Posterior Tibial Artery (PTA)
● Peroneal Artery
When these arteries are blocked, the foot is essentially starved of oxygen and nutrients. Even a small cut or pressure sore becomes a non-healing ulcer. And without intervention, that ulcer can progress to gangrene — and eventually amputation.
The critical question is: can these blocked arteries be reopened without surgery?
In most cases — yes.
What Is Peripheral Artery Angioplasty?
Peripheral artery angioplasty is a minimally invasive, image-guided procedure performed by an Interventional Radiologist. Using a tiny catheter inserted through the skin — usually at the groin or wrist — the blocked artery is accessed, and a small balloon is inflated at the site of blockage to restore blood flow.
No open surgery. No general anaesthesia in most cases. Patients typically go home the same day or within 24 hours.
The results, when performed at the right time, can be life-changing — and limb-saving.
Below are three real cases treated at ILS Hospitals, Dumdum by Dr. Jyotish Roy, Consultant Interventional Radiologist — each demonstrating how restoring arterial flow changed the outcome for diabetic foot ulcer patients.
74-Year-Old Male | Diabetic for Over 10 Years | Non-Healing Left Foot Ulcer
The Presentation:
A 74-year-old male patient with over a decade of Type 2 Diabetes Mellitus presented with a non-healing ulcer on his left foot. Despite wound dressing and standard care, the ulcer showed no signs of improvement.
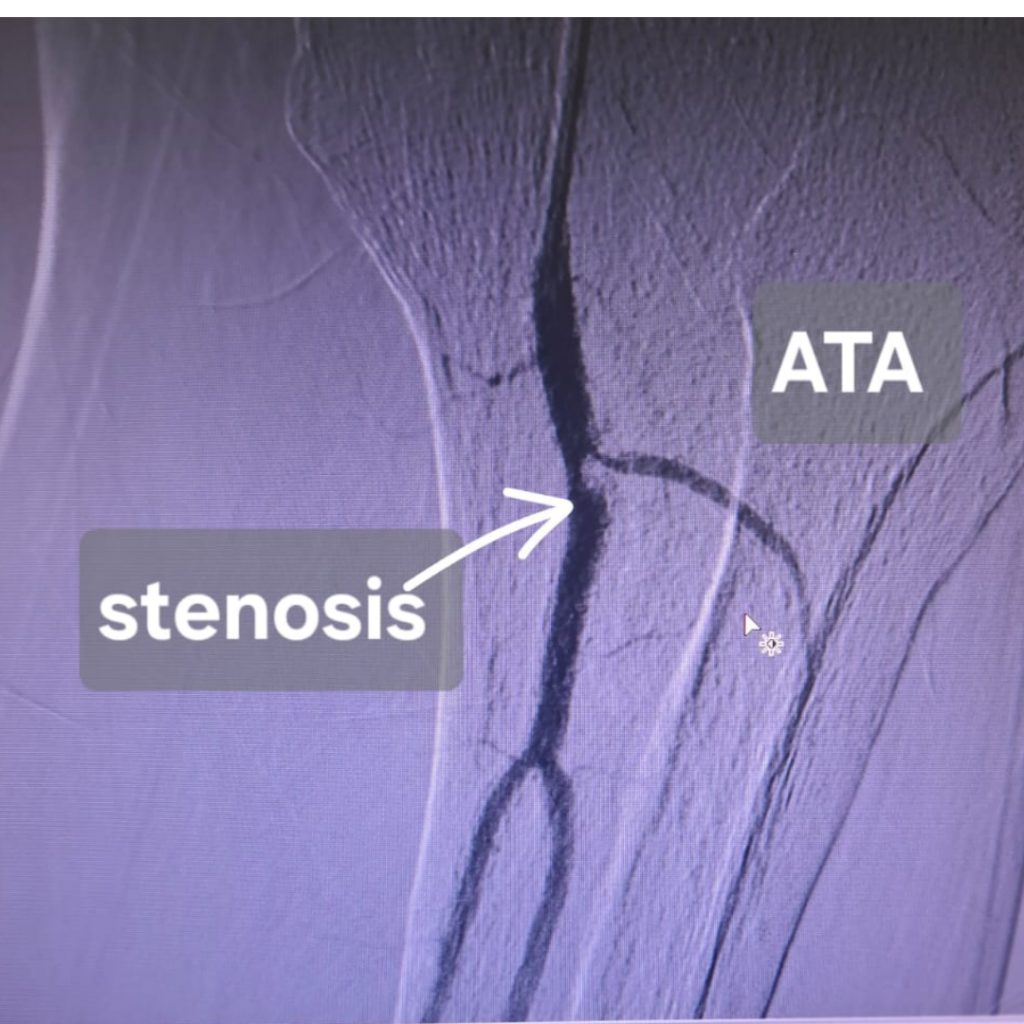
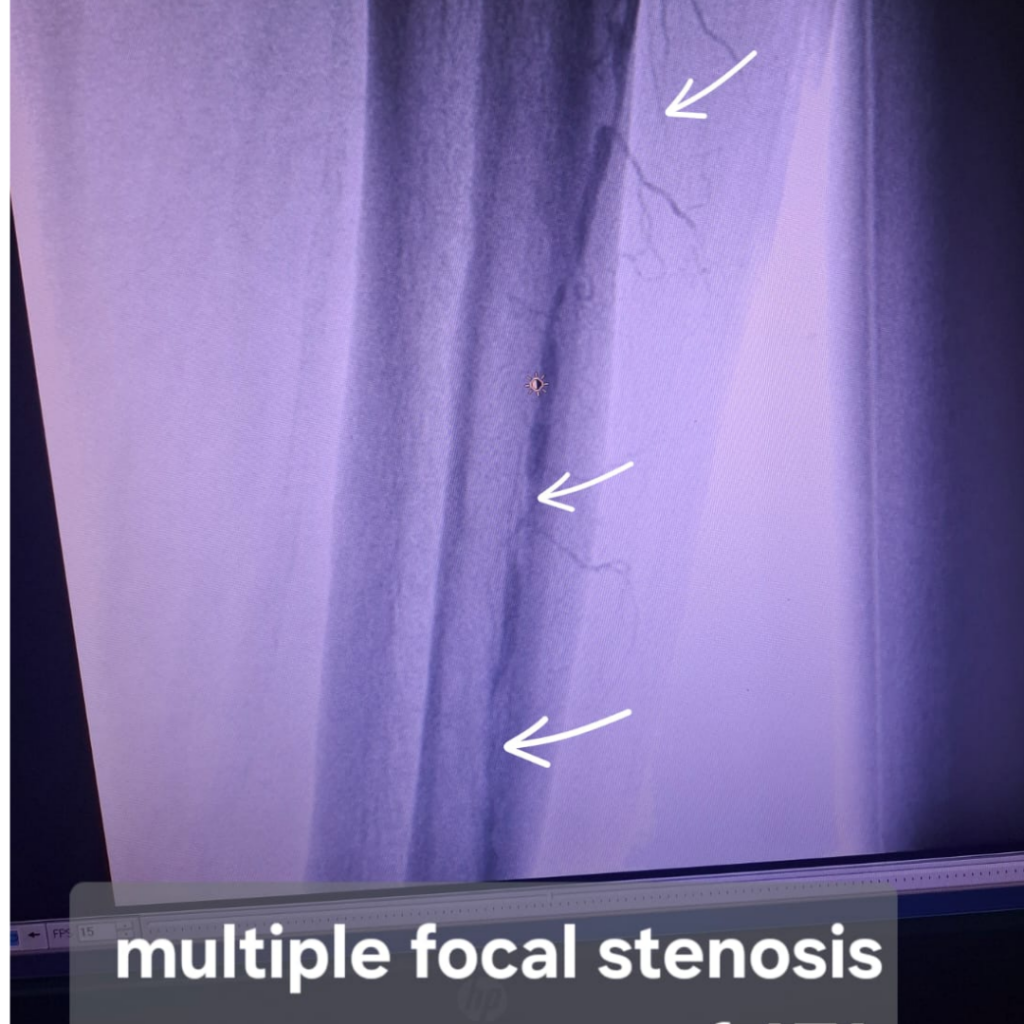
What the Imaging Revealed:
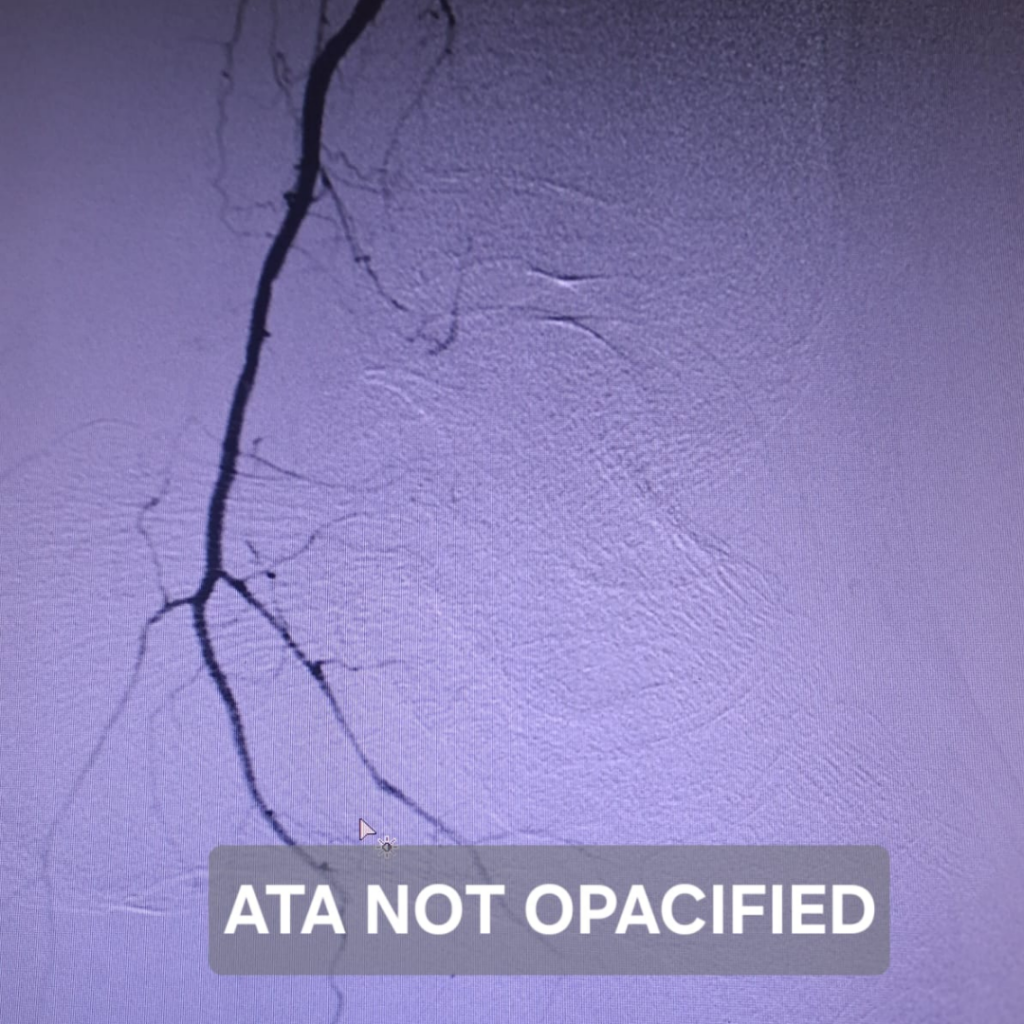
A CT Angiogram showed severe multiple stenoses (narrowings) in the left Anterior Tibial Artery (ATA), with the distal ATA and the Dorsal Pedal Artery (ADP) showing virtually no blood flow — meaning the foot was receiving almost no arterial supply.
The Intervention:
Angioplasty of the left Anterior Tibial Artery was performed. The balloon catheter was carefully navigated to the site of blockage and inflated to reopen the narrowed segments.
The Outcome:
Good flow was successfully restored to the distal ATA and ADP. Improved perfusion to the foot created the biological conditions necessary for ulcer healing — significantly reducing the risk of major amputation.
72-Year-Old Female | Diabetic for Over 15 Years + Hypertension | Non-Healing Left Foot Ulcer
The Presentation:
A 72-year-old female with longstanding Type 2 Diabetes and hypertension presented with a non-healing ulcer on her left foot. The case was particularly complex — imaging revealed not one but multiple arterial blockages.
What the Imaging Revealed:
CT Angiogram findings showed:
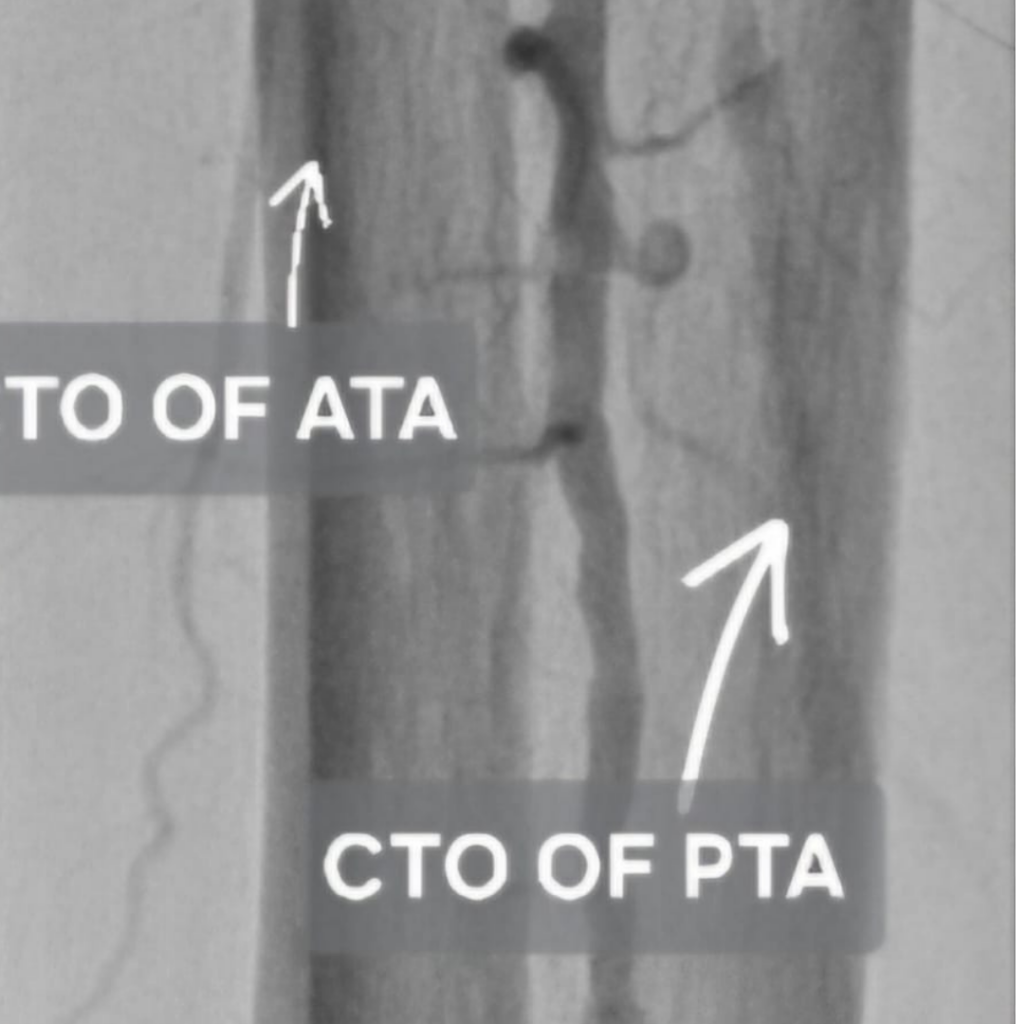
● Long segment Chronic Total Occlusion (CTO) of the Posterior Tibial Artery
● Multiple short segment CTOs in the Anterior Tibial Artery and Peroneal Artery
● Poor distal foot perfusion — the foot was surviving entirely on collateral vessels
The Intervention:
Angioplasty of the ATA and Peroneal Artery was successfully performed. Recanalization of the PTA was attempted but could not be completed due to the complexity of the occlusion.
The Outcome:
Despite partial recanalization, the improvement in distal perfusion was significant. Good blood flow to the foot was re-established via the ATA and Peroneal Artery — and with proper wound care following the procedure, the ulcer healed successfully.
This case demonstrates a crucial clinical point — even partial restoration of flow can be enough to save a limb.
82-Year-Old Male | Diabetic for 20 Years | Non-Healing Right Foot Ulcer
The Presentation:
What the Imaging Revealed:
CT Angiogram showed:
● Multiple short segment Chronic Total Occlusions (CTOs) in both the Anterior Tibial Artery and Posterior Tibial Artery
● Severe stenosis across both vessels
● Poor distal perfusion to the foot
The Intervention:
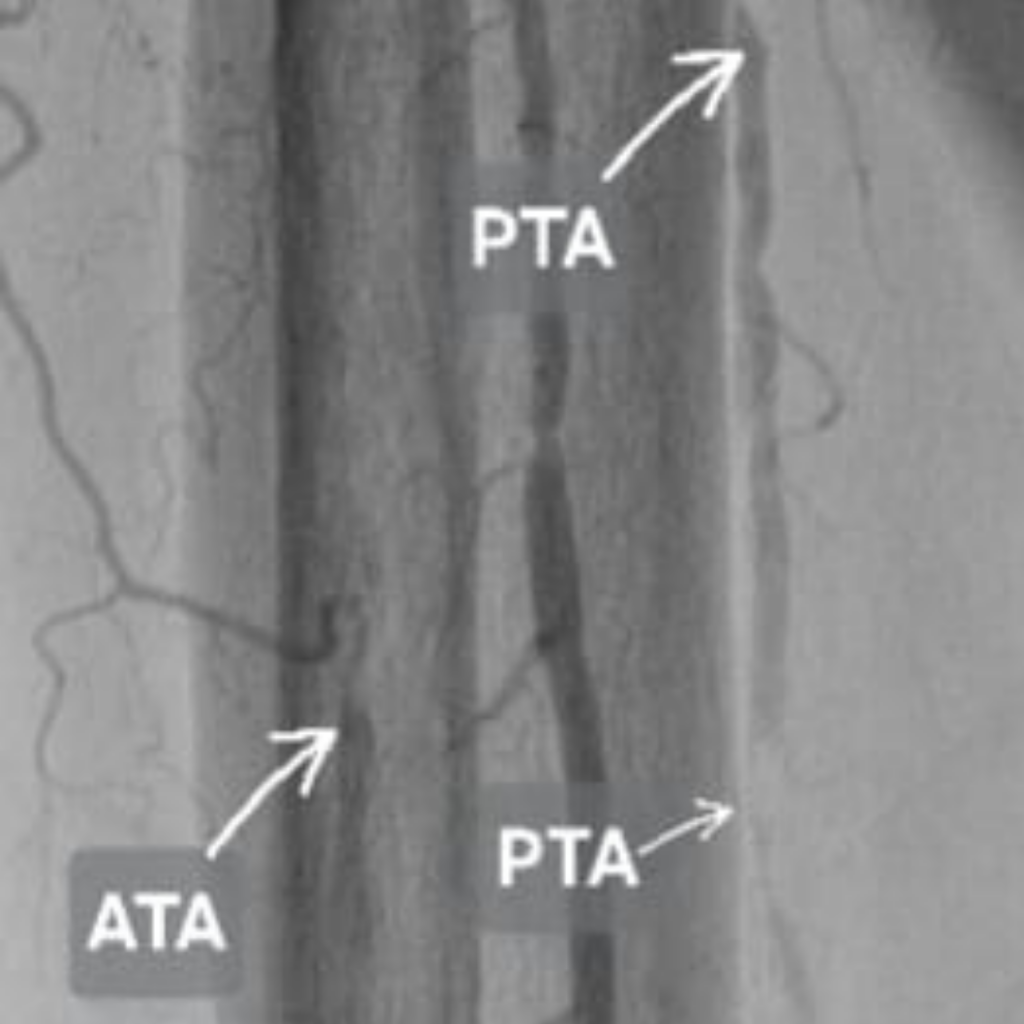
Balloon angioplasty of both the ATA and PTA was performed — successfully reopening both blocked arteries
The Outcome:
Post-angioplasty imaging confirmed good distal flow to the foot with improved perfusion to the ulcer area. The ulcer healed within 3 weeks. Limb salvage was achieved — and the patient, at 82 years of age, became ambulatory and ulcer-free, continuing on a diabetic foot care programme.
What These Three Cases Tell Us
Three different patients. Three different arterial blockage patterns. One common thread — the wound was not the primary problem. The blocked artery was.
And once the artery was reopened:
● Blood flow returned
● The ulcer received the oxygen and nutrients it needed
● Healing followed — without amputation, without major surgery
These cases also highlight something important about modern interventional radiology — even in elderly patients, even with complex multi-vessel disease, minimally invasive vascular intervention is possible and effective.
When Should a Diabetic Patient Seek Vascular Evaluation?
If you or someone in your family has diabetes, watch for these warning signs:
If you or someone in your family has diabetes, watch for these warning signs:
● A foot wound or ulcer that hasn’t healed in 2 weeks or more
● Skin darkening or blackening around the wound
● Coldness or numbness in the feet
● Pain in the legs while walking or at rest
● Absent or weak pulse in the foot
Do not wait. Early vascular evaluation can mean the difference between limb salvage and amputation.
About Dr. Jyotish Roy
Dr. Jyotish Roy is a Consultant Interventional Radiologist at ILS Hospitals, Dumdum, Kolkata, and Assistant Professor at Nil Ratan Sircar Medical College & Hospital. He specialises in peripheral vascular interventions, stroke thrombectomy, varicose vein treatment, and complex image-guided procedures.